
A Growing Demand for On-Demand Care: Perspectives from the AliveCor ECG Usability Study and the Implications on Future Cardiovascular Care Models
Rupan Bose, MD, MB, Rebecca M. Ebert, BS, Leslie A. Saxon, MD
INTRODUCTION
We now live in an on-demand era. The majority of Americans have access to almost any type of information right in their palms. It is estimated that not only do 96% of Americans own a cell phone, but approximately 81% own a smartphone (Pew Research Center, 2019). Additionally, these statistics are relatively consistent across demographics. The ubiquity of these devices, paired with an ever-growing app ecosystem, allow for on-demand access to almost any kind of personal information, including access to entertainment, finance, retail, and work data (Saxon, 2016).
This unprecedented access will change how we interact with services and workflows and recalibrate our expectations regarding data ownership. Previously, product and service offerings were at the mercy of predetermined schedules for end-consumers. Before Netflix, consumers resorted to television guides to determine when to watch a certain movie – now consumers stream at their convenience. Before Uber, consumers looked up public transportation schedules to design their trip – now consumers order rider on-demand. With this digital revolution, consumers are dictating when and how they access data instead of relying on traditional providers. However, one area that is missing from this on-demand transformation is access to personal health data and care.
However, over the last decade, the trend towards personal cardiac monitoring has changed this dynamic broadly and swiftly. Smartphone enabled Electrocardiogram (ECG) recorders have flipped the workflow of how patients self-monitor and identify concerning findings and then seek care (Bose & Saxon, 2019). These devices offer a novel way to capture cardiac metrics such as heart rate, heart rhythm, and intervals in a form factor that is seamless. Devices like the AliveCor Kardia mobile ECG device and the Apple Watch have emerged as prototypical examples of these convenient, medical-grade diagnostics that integrate with smartphones and provide long term monitoring outside the confines of brick-and-mortar clinics. Apple reportedly shipped over 30 million Apple Watches in 2019, meaning that on-demand ECG monitoring has now reached the literal hands of tens of millions of people globally (Naas, 2020).
We have seen numerous stories of patients identifying arrhythmias using these devices and then taking their recorded ECGs to a cardiologist, thus further reinforcing the value of such devices (Saxon, 2013). This contrasts previous care models where patients presented to clinic visits endorsing past symptoms that need to be investigated retroactively. As cardiovascular disease continues to be the leading cause of mortality globally, novel innovations in the diagnosis and management of such diseases using ubiquitous technologies are bound to permeate to the care models of other diseases (Mensah et al., 2019). However, in order to continue this evolution, we must continue learning what motivates patients and consumers to use these devices and incorporate these findings into future designs.
We looked back at the AliveCor Mobile Device ECG Usability Study (2013 – 2015) to better understand how people interacted with these types of devices. We wanted to understand the demographics, behaviors, levels of comfort with technology, and other characteristics of people who use such devices. We sought to better understand the implications that these devices have on patients’ ability to self-learn about their diseases and leverage those findings to design future cardiovascular care models and devices.
EARLY EXPERIENCES – THE ALIVECOR MOBILE DEVICE ECG USABILITY STUDY (2013 – 2015)
The AliveCor Mobile Device ECG Usability Study enrolled subjects into a six-month longitudinal study to understand the characteristics and behaviors of those using the commercially available smartphone enabled AliveCor Kardia ECG monitor.
Recruited subjects were consented virtually using the DocuSign platform (DocuSign, San Francisco, CA). At the time, each step was done individually. However, today, Apple’s ResearchKit platform has since emerged as a seamless way to obtain informed consent, deploy surveys, and monitor active tasks (Jardine et al., 2015).
AliveCor Kardia ECG devices were distributed to participants. Participants were taught how to capture 30-second single lead ECG rhythm strips using the device. The rhythm strips were automatically analyzed for normal sinus rhythm or an arrhythmia such as Atrial Fibrillation (AF) using AliveCor’s FDA-cleared AF algorithm (AliveCor Inc., 2014). The rhythm strips could then be uploaded to a cloud-based secure database, where they could be accessed by authorized physicians via a secure portal.
All users were sent periodic surveys throughout the six-month period. Users received a survey prior to receiving the device with questions pertaining to their background, occupation, and general behaviors around technology and medical devices. Users then received subsequent surveys at one month, three months, and six months. Survey questions pertained to device-use and behaviors. Surveys were completed virtually, and results were statistically analyzed.
Study Population
From October 2013 through December 2015, a total of 1,345 participants were enrolled into the study. Recruitment was aimed at both members of the medical community and from the general population. Of this initial group, a total of 1,166 completed the entry survey and submitted an ECG transmission. In this group, 58.1% were male, mean age was 38.2 ± 13.6 years, and 44.1% were medical professionals. The majority of participants had previously used a digital device for health monitoring (75.7%), believed it is “very important” to use digital devices to monitor health (88.2%), and stated that the use of a mobile ECG recorder would make them more conscious about their health (77.6%). Also, 71.6% reported having experienced palpitations before, and 74.3% reported never having heard of AliveCor prior to the study. Additionally, 54.2% of study participants reported ease-of-use as a strength of the device. Though this study’s average age of 38.2 appears young when compared to the expected age of patients with significant cardiovascular disease, it is comparable to the average age of the US population, which was 38.2 in 2018 (Rogers, 2019).
Use Data
A total of 28,449 ECGs were transmitted through the AliveCor Kardia mobile app during the study. On average, subjects submitted 59.7 ECG submissions over the six-month period. Nineteen subjects submitted greater than 300 transmissions. The number of ECG transmissions increased with age (Figure 1). Subjects aged 70-80 transmitted approximately 4x more ECGs per subject (158.8 transmissions/person) compared to subjects aged 30-40 (38.6 transmissions/person). Subjects working in the technology industry recorded the highest number of average ECG transmissions (78.5 transmissions/person), and subjects working in academics transmitted the fewest number (34 transmissions/person).

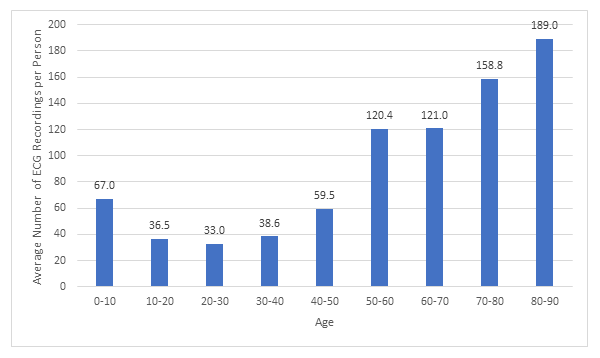
Figure 1. Average number of ECGs recorded per person over the 6-month study period by age group
By six-months, 68% of users had stopped using the device. This did not vary significantly by age, gender, or profession. Medical professionals were more likely to abandon the device earlier in the study (47% vs. 41% at one-month) and transmitted an ECG less frequently (every 12 days compared to every 7 days).
Amongst survey questions pertaining to context, the two most common settings in which ECGs were recorded were in social settings and with physical activity/exercise. This did not differ significantly between medical professionals and other subjects. Certain other settings appeared to be common reasons amongst users: 8.1% of transmissions were associated with caffeine intake, 3.9% associated with palpitations, 0.9% associated with dizziness, and 0.6% associated with chest pain. During the study, 77% of non-medical users endorsed using the device to investigate palpitations compared to 63% of medical users.
ECG Data
The average recorded heart rate (HR) was 74 beats per minute (bpm) (minimum 31 bpm, maximum 265 bpm). Bradycardia below 40 bpm was detected on 85 transmitted ECGs, and tachycardia faster than 150 bpm was detected in 255 transmissions. Mean HR declined with age as users aged 30-40 had a mean HR of 79 bpm whereas users aged 80-90 had a mean of 70 bpm (Figure 2). Male subjects had a lower average HR (70 bpm) compared to female subjects (73 bpm).
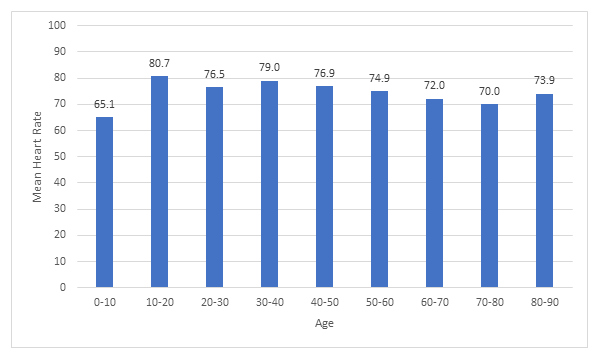
Figure 2. Mean heart rate seen in each age group
IMPLICATIONS OF HISTORICAL FINDINGS ON FUTURE DESIGNS
In this predominantly young, non-medical cohort, the findings demonstrate a tremendous appetite for on-demand ECG recordings. Subjects repeatedly used these devices to not only investigate medical symptoms, but more interestingly, used it in settings beyond the medical context such as in social settings and during physical activity. Health data has traditionally been in a silo; however, users demonstrated a collective interest in learning how their health interfaces within the greater social context.
Unsurprisingly, average ECG transmissions per person appeared to increase with age. One explanation may be that older users are more concerned about their health or may have a higher probability of symptoms that trigger a desire to record an ECG. Nonetheless, this demonstrates that older users have a significant ability to leverage technology to monitor their health. Though users in the 70-80 age group may not traditionally be viewed as technologically savvy, this study demonstrates that they are a prime audience for emerging healthcare technologies, and they deserve further studies to understand how to design experiences for them.
The results reinforced previously described “real-world” HR trends with age, as seen in previous large-scale studies. The study found an average HR of 79 bpm in subjects aged 30-40, which decreased to an average of 70 bpm in subjects aged 70-80. In the recently published data from the UCSF Health eHeart study (June 2019) with data from 66,788 subjects using smartphone photoplethysmography devices, their results found a similar average HR of 78.5 bpm in subjects aged 31-40, which decreased to an average of 73 bpm in subjects aged 71-80 (Avram et al., 2019). These results reinforce the consistency of such devices and reiterate their ability to capture meaningful data outside the clinic.
One of the challenges that came to light in this study is that 68% of users had stopped transmitting ECGs by six-months. Our interpretation of this is that despite an initial intrigue with the device and the ability to record ECGs, this novelty wears off. One possibility is that despite the device being easier to use than traditional 12 lead ECG recorders and Holter monitors, it does carry its own burdens (Barrett et al., 2014). At the time of this study, the AliveCor device was a standalone device separate from the smartphone. Perhaps carrying two devices became onerous. Another possibility is that capturing an ECG required the user to actively initiate a recording. Over time, as interest perhaps decreased, this barrier of actively initiating a recording perhaps outweighed the presumed benefit. Finally, another reason for progressively decreased usage may stem from the lack of a captivating user experience associated with recording ECGs. At the time of this study, the user experience was rather minimal – open the app, push the button to capture the recording, and then review it. In the future, a more engaging experience may be necessary to motivate users to continue recording.
The takeaways of this study are to leverage these findings to guide future designs of remote diagnostic devices. These findings indicate that devices should aim to streamline use, which can be achieved by: (1) building these ECG abilities directly into the devices that people already use daily, and (2) designing them to initiate ECG recordings in the background without requiring active initiation. We have seen steps in this direction with Apple launching the ECG feature directly on the Apple Watch, thus leveraging a device that is already a part of peoples’ daily lives. Apple has developed built-in algorithms to seamlessly detect bradycardia, tachycardia, and atrial fibrillation of these ECGs (Doshi et al., 2019). Finally, devices will need engaging experiences – which may come in the form of gamification or through improved education portals – to promote continued usage.
As these devices become more ubiquitous, these devices will change the way we manage cardiovascular disease outside the clinic. In today’s care paradigm, we as a medical community manage diseases based on episodic clinic visits, which can often occur with months or years in between. Devices like this will help clinicians obtain better insights into patients’ signs and symptoms outside the clinic, which can be leveraged to make meaningful clinical decisions and improve outcomes. These insights can also promote broadening the care model to a global, virtual care clinic where patients and physicians can make decisions together from any location (Shinbane & Saxon, 2016). It also allows for patients to learn about their clinical condition, for which, as this study shows, there is a growing interest.
ON-DEMAND REMOTE DIAGNOSTICS IN THE COVID-19 ERA AND BEYOND
At the time of writing this article, we are in the midst of the COVID-19 pandemic. The medical community is facing new challenges of how to care for patients safely, and patients are facing new challenges of how to navigate their chronic diseases. Many clinics are closed and are relying on telemedicine visits. We are realizing the challenges of traditional healthcare models that rely heavily on in-clinic practices. Additionally, patients are concerned about exposure if they enter a clinical setting. In the author’s experience, one patient had a history of intermittent palpitations, and was experiencing them during a telemedicine visit, but was hesitant to seek care. This patient is an ideal candidate to evaluate and triage using remote diagnostics. This pandemic has forced the medical community to re-evaluate each traditional in-person clinical interaction. It will accelerate the adoption of remote technologies, and we are beginning to see this as the HRS, EHRA, APHRS, LAHRS, ACC, and AHA are expected to release their upcoming “Worldwide Practice Update for Telehealth and Arrhythmia Monitoring During and After a Pandemic” guidelines (Varma et al., 2020). Additionally, the current COVID-19 clinical workflow involves self-monitoring at home and then presenting for care when needed. This model is well suited to permeate to other future workflows. In the future, patients may self-monitor cardiovascular symptoms at home with remote monitoring devices and then present as needed, as opposed to fixed-interval clinic visits.
As the global medical community is forced to learn how to treat this novel virus, these devices offer a rapid method to deliver care and conduct novel research. Initial studies have shown the importance of inpatient QT monitoring when treating COVID-19 patients with potential QT-prolonging or arrhythmogenic medications such as hydroxychloroquine and azithromycin (Chang et al., 2020; Roden et al., 2020). However, as more patients are deemed stable for continued care at home, there will be an increased focus on studying patients in the outpatient setting using mobile devices. In light of this, AliveCor received FDA clearance to use their mobile six-lead personal ECG device to monitor QT durations in patients outside the hospital (AliveCor Inc., 2020). As the global medical community studies this in parallel, a new large-scale decentralized approach to collecting research data will emerge leveraging remote diagnostics to collect data from any person in an any location. Thus, remote diagnostics are quickly emerging out of necessity to become a key foundation in the way we do research and manage patients in an increasingly remote telemedicine-based healthcare paradigm.
CONCLUSIONS
There is a growing demand for on-demand healthcare. In a time when consumers have on-demand from all other industries, yearly clinical check-ins are far from sufficient. Rather, devices like this will fill the gap and quench the demand for healthcare. Consequently, a new paradigm of continuous measurement and self-learning will emerge and drive the future of cardiovascular disease management, aided by the rise of remote diagnostic devices.